
Last Updated on February 12, 2024
Medical Advice Disclaimer: This article is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other qualified healthcare provider regarding a medical condition or treatment.
Suppose you enjoy alcohol but find it’s starting to harm your overall well-being.
Is your first thought that alcohol has bled you of “all self-sufficiency and all will to resist its demands”? Or do you look at alcohol as something you can moderate with the right techniques?
Alcoholics Anonymous (A.A.) created the idea that problem drinking equals powerlessness over alcohol and requires its removal from your life. And in the almost 100 years since A.A.’s founding, this idea has helped millions achieve sobriety.
But is total abstinence the only solution? Many leading professionals in the study of alcohol abuse say no.
Today numerous treatment options help problem drinkers moderate consumption and live a healthier life. Many of these options were crafted by clinicians who saw that A.A. didn’t work for everyone. But which is right for you? Keep reading to find out.
The History of A.A.
A.A. was founded in 1935, the same year the first can of beer was sold in Richmond, VA. A stockbroker and a surgeon, each convinced they were drinking too much, decided to pool their resources to help other problem drinkers.
Bill W., the stockbroker, and Dr. Bob S., the surgeon, had both been affiliated with the Oxford Group, led by an Episcopal clergyman. Bill credited the New York chapter of the Oxford Group with helping him achieve sobriety, though others in the chapter struggled. Bob, a member of the Akron, OH chapter, struggled as well.
When they finally met, Bill convinced Bob that excess alcohol use was a disease needing treatment. Bob, despite his medical credentials, had never looked at his drinking problem this way. Together, armed with the spiritual and medical resources of the time, they began working with problem drinkers at Akron’s City Hospital, and A.A. was born.
By the end of 2021, A.A. had 1.97 million members worldwide — a drop of 8.3% from 2020. 2021’s totals are roughly the same as their membership tally at the end of 1997.
While still on firm footing, A.A.’s lack of sustained growth might signal that it works for many, but not for all.
The Twelve Steps of A.A.
A.A. is a mindset, not a clinical regimen. This mindset is the product of A.A.’s famous Twelve Steps, laid out by co-founder Bill W. in one of his early books.
A.A.’s website makes it no secret that the Twelve Steps “are a set of spiritual principles. When practiced as a way of life, they can expel the obsession to drink and enable the sufferer to recover from alcoholism.”
This bold promise of recovery attracted legions of individuals to A.A. meetings.
Alongside A.A.’s rapid growth, the American Psychological Association (APA) was also studying the problem of alcohol abuse. In 1952 they published their findings and recommendations in the first edition of The Diagnostic and Statistical Manual of Mental Disorders (DSM). Contributors to this publication began to recognize that not all drinking problems were equally severe, opening the door to more diverse treatment options.
But before the DSM gained wide acceptance, the Twelve Steps were the only lifeline for problem drinkers:
1. We admitted we were powerless over alcohol — that our lives had become unmanageable.
This Step asks the drinker to come to grips with their alcoholism, a term used heavily in A.A.’s literature. Unless the drinker admits they have this all-or-nothing disease, A.A. will not work for them.
Since A.A.’s founding, the DSM-5 no longer considers the term “alcoholism” sufficient to explain problem drinking. Instead, the DSM-5 uses the term “alcohol use disorder” (AUD) with three degrees of severity: mild, moderate, and severe.
Medical professionals today help the drinker understand the severity of their problem and suggest a personalized recovery plan.
2. Came to believe that a Power greater than ourselves could restore us to sanity.
Once the drinker admits defeat, the next step is to lean on an external “Power” to help lift them out of their situation.
3. Made a decision to turn our will and our lives over to the care of God as we understood Him.
This Step gives the more open-ended term “Power” an explicitly religious name (“God.”) But in an A.A.-approved pamphlet for atheist and agnostic members, the first sentence is “A.A. is not a religious organization.”
The pamphlet goes on to qualify “God” or “Power” as anything that “helps us find an inner strength that we were previously unaware of.” Recovery depends on tapping that inner strength, whatever its source.
4. Made a searching and fearless moral inventory of ourselves.
Part of recovery hinges on identifying how the sufferer’s alcohol use has harmed others.
5. Admitted to God, to ourselves, and to another human being the exact nature of our wrongs.
A.A. meetings are popular forums for sufferers to admit their failings, both to themselves and others.
6. Were entirely ready to have God remove all these defects of character.
Again, recovery means handing over some or all agency to God or whatever the sufferer considers their Higher Power.
7. Humbly asked Him to remove our shortcomings.
In this religiously worded Step, the sufferer must pray to or rely on their chosen Power to erase their moral failings.
8. Made a list of all persons we had harmed, and became willing to make amends to them all.
It’s not enough to identify those harmed from alcohol abuse. The sufferer must confront those affected and make amends.
9. Made direct amends to such people wherever possible, except when to do so would injure them or others.
This Step acknowledges that some of the wounds caused by alcohol abuse are too deep for a one-on-one reconciliation.
10. Continued to take personal inventory and when we were wrong promptly admitted it.
A sufferer must take “personal inventory” throughout the recovery process, not just at the beginning. When A.A. members in recovery stumble, they must make amends as best they can and recommit to abstinence.
11. Sought through prayer and meditation to improve our conscious contact with God as we understood Him, praying only for knowledge of His will for us and the power to carry that out.
Belief in a Higher Power isn’t enough for recovery. The sufferer must engage with this Power to draw strength from it during recovery.
12. Having had a spiritual awakening as the result of these Steps, we tried to carry this message to alcoholics, and to practice these principles in all our affairs.
This final Step re-emphasizes the spiritual roots of A.A. and affirms the relevance of the Twelve Steps in everyday life. In other words, recovery is not a one-time event. The sufferer who chooses the A.A. path must follow the Twelve Steps for a lifetime in order to maintain recovery.
At face value, the Twelve Steps leave little room for nuance. There is no assumption that problem drinking has levels of severity, or that individuals who struggle with belief in God or a Higher Power have any chance of recovery.
Who is A.A. for?
As members of the Oxford Group, it’s no surprise A.A. founders Bill W. and Dr. Bob S.’s Twelve Steps have a strong spiritual — if not religious — outlook. But the founders never expected A.A. members to share these convictions.
The A.A. pamphlet for atheists and agnostics names “the desire to stop drinking” as the single membership requirement.
Is A.A. a cult?
For those seekers still unsure about the use of “God” and “Higher Power,” the pamphlet includes a 1965 statement from Bill W.:
“The full individual liberty to practice any creed or principle or therapy whatever should be a first consideration for us all. Let us not, therefore, pressure anyone with our individual or even our collective views.”
So Bill W. and Dr. Bob S. never intended A.A. to be a cult-like haven for problem drinkers with a religious bent. They cast their net much wider.
But since A.A. has no policy-making central authority, some local A.A. meetings might stress religion more than others.
A.A. and Modern Medicine
Despite its spiritual backbone and friction with the DSM, many prominent addiction specialists still recommend A.A.
Harvard Medical School professor Dr. John Kelly argued in 2020 that “having an engaging, widely available, and free recovery-specific support option like A.A. can help sustain behavioral changes” in AUD sufferers.
Kelly doesn’t claim A.A. is the only or best solution. But it can benefit those who want the support of others as they seek recovery.
Do I need A.A.?
A.A. is worth a look by anyone who wants to explore total abstinence from alcohol as a way to regain control over their life. The organization offers a twelve-question self-assessment to help you might have a drinking problem.
Plus the wide availability of free meetings makes A.A. a reasonable place to start. A.A.’s website makes it easy to find nearby meetings.
Nate Kelly, who found recovery through A.A. and now hosts the podcast The Sobriety Diaries, recommends it if you share these traits:
- Craves a sense of belonging. A.A. provides a community of individuals who understand the struggles of addiction, offering a sense of belonging and support.
- Values anonymity. A.A. is built on the principle of anonymity, allowing individuals to share their experiences without fear of judgment or disclosure.
- Responds well to peer support. Many find strength in the shared stories and support offered by fellow A.A. members.
- Seeks structure. A.A. offers a structured program and steps to guide individuals toward recovery.
- Is open to the spiritual aspect. Nate never felt pressured to define his Higher Power in a particular way. For him, “My Higher Power is the universe, Mother Nature, natural vibrations and the force fields that pull us exactly where we are supposed to be each day and I think of it in a more scientific way.”
But if you still feel uncomfortable committing to A.A., other treatment options exist. First, it’s important to understand how severe your problem might be.
A good place to start is the DSM-5’s eleven criteria for alcohol use disorder. If five or fewer criteria apply to you, your attachment to alcohol is moderate or mild. For example, it’s a warning sign of AUD if you’ve “wanted a drink so badly you couldn’t think of anything else.”
Sunnyside is one of several online communities that can help mild or moderate alcohol use disorders from getting worse. Or as psychotherapist Katherine Bonham puts it, Sunnyside can “help you identify if you can achieve a healthy relationship with alcohol or if you need to abstain completely.”
Solutions like Sunnyside let you set weekly goals for reduced consumption, and a team of coaches helps keep you on track without any shame or judgment.
How effective is A.A.?
The foreword to the 1955 second edition of A.A.’s Big Book claims a success rate of 75% for members who went to meetings and “really tried.” Of those, half achieved sobriety immediately, and 25% became sober eventually. The remaining 25%? They “showed improvement.”
Again, recovery for A.A. means total abstinence from alcohol. A sustained reduction in consumption would not count as success.
Does A.A. even work?
Without taking anything away from A.A.’s early success, retired Harvard Medical School professor Dr. Lance Dodes, writing in 2015, found A.A.’s sobriety rates were trending down. In The Sober Truth he studied A.A.’s rates of retention and member involvement. Dodes estimated an A.A. success rate of between 5% and 10%.
But this low success rate didn’t stop Dr. Keith Humphreys, a Stanford professor, from evaluating 57 existing studies on A.A.’s effectiveness. In his 2020 report, more than half the 57 studies passed Stanford’s criteria for quality.
Humphreys “nearly always found [A.A.] to be more effective than psychotherapy in achieving abstinence,” based on the approved studies. Results were consistent among young, elderly, male, female, veteran, and civilian patients.
And even if you’re still deciding whether abstinence is right for you, Katherine Bonham calls A.A. a “great option for many people looking for community and accountability.”
The point is A.A. still works for some, amidst enormous advances in the study and treatment of addiction disorders. But it’s still worth asking why A.A.isn’t more successful.
Why is A.A. not more effective?
If Dodes is correct, and 90% of A.A. members fail to achieve sobriety, then where might the program be falling short?
One Size Does Not Fit All
One issue might be A.A.’s “one size fits all” approach. The only path to sobriety is wholly embracing the Twelve Steps and attending meetings.
But the roots of alcohol abuse often stem from genuine mental-health disorders. Katherine Bonham notes, “I’ve rarely seen someone in my career who doesn’t have underlying mental health struggles connected to alcohol misuse.”
Trained psychologists often don’t lead A.A. meetings, which can disadvantage this set of problem drinkers. Cognitive behavioral therapy or some other intervention might be a better fit for these individuals than A.A.
Identifying as an “Alcoholic”
Another problem with A.A. might be the pressure it puts on problem drinkers to “overidentify” as “alcoholics.”
The point here isn’t to minimize the dangers of severe physiological or psychological alcohol dependence. These drinkers might be alcoholics, and their health can decline quickly.
But not all drinkers are truly dependent. Clinical psychologist G. Alan Marlatt suggests it’s not helpful for everyone to identify as an “alcoholic” and take on the shame that goes with it.
Marlatt suggests looking at excess consumption as a bad habit that good habits can replace over time. Saying “I’m an alcoholic” is much less helpful than “I engage in certain behaviors that have certain negative consequences and these behaviors can be changed.”
A 2014 study from the Centers for Disease Control and Prevention (CDC) supports Marlatt’s claim. It found that “nine in ten adults who drink too much alcohol are not alcoholics or alcohol dependent.” So it may be worth encouraging problem drinkers to develop better habits.
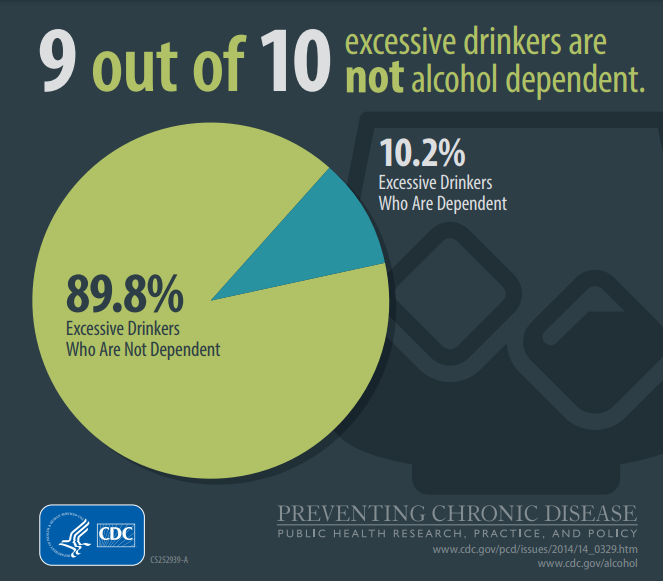
Source: CDC
Dr. Adi Jaffe, author of The Abstinence Myth, understands it’s difficult to eradicate bad habits. Messing up is an expected part of the process and shouldn’t be a source of shame. The goal is to keep trying until the drinker finds balance.
Can A.A. be a tool for moderation?
Bill W. and Dr. Bob S. believed abstinence was the only solution for someone with a confessed drinking problem. A single drink, they thought, almost guaranteed a severe relapse.
A.A.’s introductory pamphlet doesn’t mince words: “For an alcoholic, one drink is too many and a thousand are not enough.” In other words, moderation doesn’t fit A.A’s definition of recovery.
Sobriety vs. Moderation
But say a new A.A. member who averages five daily drinks manages to abstain for six days before having one drink on the seventh. This one drink would qualify as a failure in the A.A. model, which might demoralize the sufferer and lead to heavier drinking. Abstaining for six days would not qualify as a “small victory” or “positive step towards recovery.”
That single drink would also be a sign that the individual isn’t giving their all to A.A.’s program. And A.A. doesn’t have much empathy for those who can’t or won’t abstain completely. Chapter 5 of the Big Book states,
“Those who do not recover are people who cannot or will not completely give themselves to this simple program, usually men and women who are constitutionally incapable of being honest with themselves.”
Many drinkers would claim that “being honest with themselves” brought them to A.A. in the first place. And the thought of being “constitutionally incapable” of self-honesty? That might trigger a more severe relapse than having that single weekly drink.
What are some A.A. alternatives?
So while A.A. is still a valuable resource for problem drinkers, those seeking to moderate might want to look elsewhere.
Sinclair Method
The Sinclair Method is one of many forms of harm reduction. As the name suggests, the goal here is to reduce alcohol’s harmful effects without necessarily curtailing consumption.
Named after the doctor who popularized it, the Sinclair Method reduces the desire to drink with the aid of Naltrexone, an endorphin-blocking drug that blocks the pleasure associated with alcohol consumption. When the brain stops associating alcohol with pleasure, reduced cravings and better control should result.
Physicians who administer the Sinclair Method frequently recommend counseling in tandem with Naltrexone use.
According to addiction specialist Dr. William Nelson, the Sinclair Method has an 80% success rate in clinical studies and “in the clinical experiences of hundreds of our patients over the last five years.”
Cognitive Behavioral Therapy (CBT)
CBT rests on the idea that psychological problems stem from incorrect thought patterns and unhealthy, learned behaviors. Alcohol abuse may have its origin in thoughts such as “I’m a failure” or “I’m not loveable.”
Once the sufferer sees the error in their patterns of thought, they’re in a better position to confront the role of alcohol as a coping mechanism.
According to the National Center for Biotechnology Information, CBT “has been extensively researched and found to be effective in a large number of outcome studies for psychiatric disorders including … substance abuse.”
“Mindful” Alcohol Consumption
Mindful drinking teaches problem drinkers how to recognize alcohol cravings and cope with them in a healthy way. It can complement traditional 12-step recovery programs or be the sole solution for those looking to reimagine their relationship with alcohol.
Say you set a daily goal of one glass of wine but want more. Mindfulness helps you pause before giving in, which takes the edge off the urge and makes it easier to manage.
For UCLA professor Dr. Hrishikesh Belani, mindfulness acknowledges that a healthy lifestyle doesn’t always have to exclude alcohol consumption:
“By being mindful about when/how/where and what they drink they can sort of maximize any benefit of drinking (gustatory, social, celebratory, reward, etc.) while minimizing and short, near and long term negative effects (hangover, sleep, behavioral, weight gain, blood pressure, and other organ damage, etc.).”
Here are some popular and effective practices that encourage mindfulness:
- Journaling helps drinkers chronicle their relationship with alcohol and reflect on situations where they’re tempted to drink more. They can develop strategies for moderating consumption when these situations come up.
- The Calm app teaches meditation and relaxation techniques. Drinkers can use it to manage stress, rather than reach for a beer.
- Moderation Management offers online resources and support groups for anyone seeking to limit their alcohol consumption.
- Sunnyside is like the Calm app, but for alcohol health. It teaches drinkers how to enjoy life more without completely eliminating alcohol. Users track their number of drinks, and online coaches offer tips for reduction along the way. And if a user stumbles, Sunnyside coaches never judge or criticize, but encourage a fresh start.
Interview with Nate Kelly on Experience with A.A.
Nate Kelly is a podcasting pro, published author, and public speaker. He’s also a recovering alcoholic who found success with A.A. His podcast The Sobriety Diaries shares inspiring stories of recovery for those seeking to reduce their consumption.
When is A.A. a good fit for someone struggling with alcohol use disorder?
A.A. can be a great fit for someone struggling with alcohol use disorder when they seek a supportive community and a structured program to help them achieve and maintain sobriety.
It’s particularly effective for individuals who are open to a 12-step approach and benefit from sharing their experiences with others who have faced similar challenges. However, it’s important to remember that A.A. is just one option among many, and what works best can vary from person to person.
However, it’s important to acknowledge that A.A. isn’t a one-size-fits-all solution. Its effectiveness varies from person to person. I’ve realized for ME it’s been effective because I am someone who:
1. Craves a sense of belonging: A.A. provides a community of individuals who understand the struggles of addiction, offering a sense of belonging and support.
2. Values anonymity: A.A. is built on the principle of anonymity, allowing individuals to share their experiences without fear of judgment or disclosure.
3. Responds well to peer support: Many find strength in the shared stories and support offered by fellow A.A. members.
4. Seeks structure: A.A. offers a structured program and steps to guide individuals toward recovery.
5. Is open to the spiritual aspect: The 12-step approach includes a spiritual component that can be meaningful for those who embrace it.
When is A.A. not a good fit?
A.A. may not be the best fit for everyone, and there are situations where it might not align with an individual’s needs and preferences. I have spoken to individuals who didn’t find A.A. helpful based on:
1. Non-Spiritual or Non-Religious Beliefs: A.A. incorporates a spiritual or Higher Power element into its program, which can be a challenge for individuals who don’t have religious beliefs or who have strong objections to spiritual aspects.
2. Desire for Moderation: If someone’s goal is to reduce their alcohol consumption rather than achieve complete abstinence, A.A., which promotes lifelong sobriety, may not align with their objectives.
3. Alternative Recovery Philosophies: Some people resonate more with alternative recovery philosophies like harm reduction, mindfulness-based approaches, or secular recovery groups. A.A.’s 12-step approach may not match their preferred recovery framework.
4. Past Negative Experiences: Individuals who have had negative experiences with A.A., such as feeling judged or unsupported, may not find it a good fit for their recovery journey.
5. Lack of Accessibility: In some regions, A.A. meetings may not be readily available, or the scheduling may not align with an individual’s commitments and lifestyle.
6. Need for Specialized Treatment: Some individuals may have co-occurring mental health disorders or complex medical needs that require specialized treatment beyond what A.A. provides.
7. Preference for Evidence-Based Approaches: A.A. is not a clinical or evidence-based treatment program. Some individuals may prefer therapies or treatments with a strong empirical foundation.
When you were going through A.A., was the God / Higher Power dynamic a stumbling block? Why or why not?
For me it wasn’t a stumbling block. I didn’t grow up in a particularly religious or spiritual household and, as a gay man, hadn’t really followed up with Jesus in a minute.
However, when I entered treatment, I knew that whatever I had been doing wasn’t working and I was willing to try anything else. My first day in detox was brutal and when my roommate dragged me down the hall to a “meeting” I had NO idea what to expect and didn’t realize that my life was about to change forever.
When I first heard “Higher Power” and that it could mean whatever was helpful to each individual, I took that to heart.
My Higher Power is the universe, Mother Nature, natural vibrations and the force fields that pull us exactly where we are supposed to be each day and I think of it in a more scientific way. This helps me to understand and believe that I am guided in a more natural and spiritually driven way as opposed to anything “religious.”
Weird? Maybe. Has it kept me sober for 8 years (in addition to other things)? Absolutely.
Were you aware of alternatives for AA that were moderation or mindfulness focused when you went through the program?
Before entering treatment, I was blissfully unaware of other forms of treatment other than the traditional in-patient detox and follow up A.A. participation.
However, over the last 8 years (that’s a miracle even saying that) I have come to learn of several based on my conversations with guests on The Sobriety Diaries:
1. Moderation Management: Moderation Management is a program designed for individuals who want to moderate their drinking rather than abstain completely. It emphasizes self-monitoring, goal setting, and responsible drinking.
2. SMART Recovery: SMART Recovery is a science-based program that offers tools and techniques for individuals struggling with addictive behaviors. It focuses on self-empowerment, cognitive-behavioral strategies, and goal setting, providing a more cognitive and practical approach to recovery.
3. Mindfulness-Based Sobriety: Mindfulness practices, such as mindfulness-based relapse prevention (MBRP), have gained popularity as complementary approaches to traditional recovery programs. These techniques help individuals develop awareness of cravings and triggers and use mindfulness to cope with them.
4. Harm Reduction Programs: Some organizations and communities embrace harm reduction principles, which prioritize reducing the negative consequences of substance use rather than total abstinence. These programs often provide resources for safer use and education.
Awareness of these alternatives has grown over time, offering individuals more choices to tailor their recovery journeys to their specific needs and preferences. It’s essential to explore these options and consult with professionals to determine the best approach for one’s unique circumstances.
But what do the medical experts have to say?
Dr. Hrishikesh Belani is Associate Medical Director of the South Los Angeles Health Center Group.
1. Please provide the most authoritative statistic you’ve seen about the success rate of A.A. (with a link, if possible).
In 2020 a systematic review of AA and other 12-step programs was published in the Cochrane Library. It summarizes the results of multiple studies and trials. Looking at all randomized trials comparing AA and 12-step to other clinical interventions, 12-step did seem to improve rates of continuous abstinence, percentage days abstinent, and at 12, 24 and 36 months out.
2. Why do you think A.A. isn’t more successful, given its global footprint?
AA emphasizes the role of a higher power, and some people do not prefer this in a mutual help solution. Some do not relate to (or are not prepared to process) the group dynamic or stories shared and the milieu can be more depressing than motivational.
3. What have you seen be most effective when it comes to alcohol harm reduction?
Anecdotally, nonalcoholic replacements that are similar in look, feel and flavor to alcohol-containing beverages help facilitate “safer use” of alcohol by making it easier to cut back. People can consume just those or a mix of those and alcoholic beverages without changing too many behaviors.
Medications for alcohol use disorder like naltrexone, acamprosate, gabapentin, and topiramate are ultimately treatments but do not have to be used exclusively to achieve abstinence.
These are harm reduction solutions related to safer use by an end user, there are other public health and system/structural tools and interventions that achieve harm reduction related to alcohol use.
4. Why do you think tools like Sunnyside that focus on habit change/mindfulness could be a step towards long term solutions around alcohol health?
Sunnyside allows users to set goals and define the purpose alcohol serves in their lives. Usually, it allows people to realize they can get much more out of much less consumption.
By being mindful about when, how, where, and what they drink, people can maximize enjoyment of alcohol while minimizing short-, near-, and long-term negative effects. These effects include hangovers, sleep problems, weight gain, high blood pressure, and organ damage.
Is moderation really possible?
Moderation is indeed a solution for many who seek a healthier lifestyle without resorting to total abstinence. But again, there is no “one size fits all” solution.
A 2011 study in the Journal of Consulting and Clinical Psychology found that “non-dependent problem drinkers” may benefit from online moderation programs. The study cites programs encouraging this set of drinkers to “set goals, self-monitor their behavior, and get detailed feedback on their progress based on their input.”
But how do you know whether you’re a non-dependent problem drinker? If in doubt, Katherine Bonham suggests starting with individual therapy. A therapist can help you find the right treatment option or options given your condition. And one of those options might be A.A.
Start Your Moderation Journey with Sunnyside
If you believe that reducing but not eliminating alcohol use is consistent with a healthy, fulfilling life, try moderation programs like Sunnyside. In a 2023 survey of Sunnyside members, 81% report they could better manage alcohol cravings, and 96.7% report less drinking overall.
Start exploring moderation today. This 3-minute quiz will personalize an alcohol reduction plan you can manage from your phone. Your long-term health and well-being is worth it.
References
Chand SP, Kuckel DP, Huecker MR. Cognitive Behavior Therapy. [Updated 2023 May 23]. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
https://www.ncbi.nlm.nih.gov/books/NBK470241/
Hester, R. K., Delaney, H. D., & Campbell, W. ModerateDrinking.Com and moderation management: Outcomes of a randomized clinical trial with non-dependent problem drinkers (2011). Journal of Consulting and Clinical Psychology, 79(2), 215–224. https://doi.org/10.1037/a0022487
Mindfulness and metaphor in relapse prevention: An interview with G. Alan Marlatt (1994).
Journal of the Academy of Nutrition and Dietetics 94(8), 846-848.
https://doi.org/10.1016/0002-8223(94)92361-2
Single E. Harm Reduction as an Alcohol-Prevention Strategy. Alcohol Health Res World. 1996;20(4), 239-243.



